The programme is essentially the same for children & adults alike.
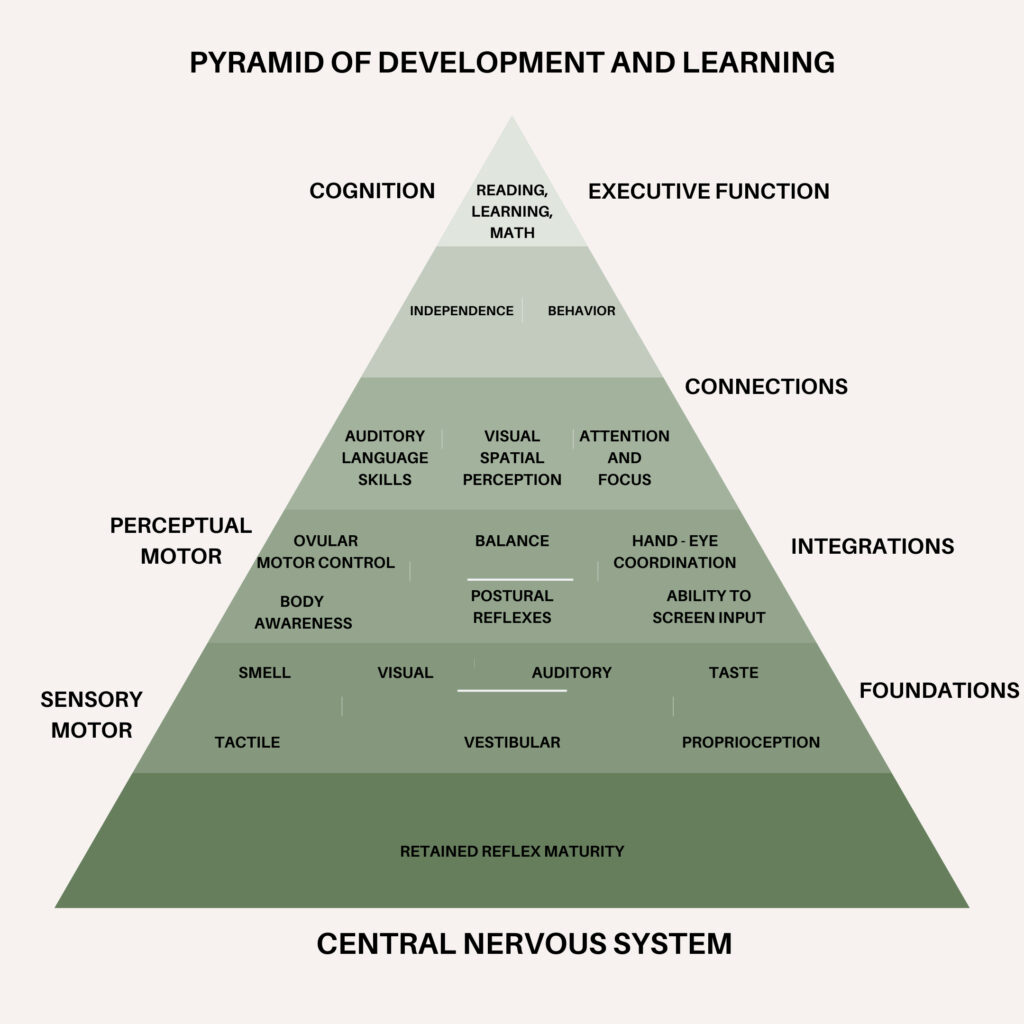
Establishing whether the reflexes have been retained determines whether NDT is appropriate for you or your child. These reflexes are designed to programme the brain in areas such as balance, co-ordination, eye movement/tracking and appropriate production of adrenaline – therefore it is possible to assess these areas of function for evidence that the Central Nervous (CNS) is immature. We are able to do this either in clinic (face-to-face) or remotely (via videocall).
Initial consultation
This is for 60 minutes.We will take a comprehensive case history and discuss symptoms and areas of concern. We perform a series of tests to identify the presence of any relevant reflexes. These involve balance and co-ordination tests that most children enjoy very much – there are no academic or medical tests – simply, we are assessing the individual’s functioning CNS.
Treatment programme
If, during the assessment, we establish evidence of the primitive reflexes being retained, we can begin a programme of neural stimulation. We provide detailed and clear instructions – whether this be skin stimulation, movement exercises or sound therapy, all of which are carried out at home.
Review
Generally, we review every 4-8 weeks and make adjustments and changes to the programme as needed. Typically, we review remotely via videocall (your child doesn’t necessarily need to be present) and then when appropriate, we retest the reflexes to check our progress (again, this can be done in clinic or remotely).
The aim of the treatment programmes are to reproduce the movement and self-stroking stimulation that the baby should have been making at the point of the developmental interruption, either in utero or during the first few months after birth. Essentially we take the CNS back to a point where the domino run of reflexes originally halted and restart the process by mimicking the processes that should have happened at these key developmental stages.
We supply a small, specific soft brush to carry out the stimulation of specific areas of the face, hands, back and torso; this takes no more than 5 minutes twice a day. We may also teach specific movements designed to recreate certain post–birth movements that the baby should have been making to carry out and complete its own development. We also use the Johansen IAS programme which is an auditory stimulation technique that makes it possible to further target the specific speech and language areas of the cortex.
A programme will last on average 9-12 months – then we take a break which enables us to assess the lasting and continued development of the CNS. It is sometimes necessary to ‘tidy up’ any remaining areas of function with specific, targeted programmes following the period after the break from treatment.
Fundamentally, the programmes act to inhibit the retained primitive reflexes and to allow the more appropriate, adult reflexes to develop as the CNS matures.
Neuro Developmental Assessment (with Report)
In addition to assessing primitive reflexes, we also offer a full Neurodevelopmental reporting assessment. During this 90minute appointment, in addition to assessing primitive reflexes, we also perform an Audiogram to test Auditory processing. At the end of this process you will receive a report document that fully details the assessment, it’s outcomes, what they can mean and how we prioritise next steps and the support process.
This assessment can only be delivered in person so do consider whether you feel your child could engage in the process comfortably. This consultation is often the best choice for families who are on a diagnostic or assessment pathway, presenting evidence for an EHCP, or simply want a tangible assessment report of their child’s neuro development.